
Pharmacogenetics and pharmacogenomics (abbreviated together as PGx) are key to the future of personalized medicine. Pharmacogenomic biomarkers provide tools to predict (a) drug response or (b) adverse drug reactions. Such biomarkers help to maximize efficacy and minimize toxicity.
The evolution of pharmacogenomic biomarkers in oncology is the direct offshoot of targeted drug development of imatinib (Gleevec), a specific inhibitor of BCR-ABL kinase, for chronic myelogenous leukemia (CML) and trastuzumab (Herceptin) for metastatic breast cancer. BCR-ABL kinase is expressed by a fusion gene on Philadelphia chromosome. Philadelphia chromosome is a result of reciprocal translocation of DNA resulting in the fusion of cABL (on chromosome 9) and BCR (on chromosome 22). Presence of BCR-ABL in CML leukocytes and over-expression of Her2/neu receptor in breast cancer are the examples of validated pharmacogenomic predictive biomarkers.
The Jargon (definitions from NCI dictionary)
Biomarker (BY-oh-MAR-ker) is a biological molecule found in blood, other body fluids, or tissues that is a sign of a normal or abnormal process, or of a condition or disease. A biomarker may be used to see how well the body responds to a treatment for a disease or condition. Also called molecular marker and signature molecule.
* Predictive biomarker predicts patient’s response to a drug, and prognostic biomarker predicts the recovery from a disease/cancer.
Pharmacogenomics (FAR-muh-koh-jeh-NOH-mix) is the study of how a person’s genes affect the way he or she responds to drugs. Pharmacogenomics is being used to learn ahead of time what the best drug or the best dose of a drug will be for a person. Also called pharmacogenetics.

The List
Recently, Nathan Nagel of Oncology Pharma, London, U.K., posted a list of oncology focused pharmacogenomic biomarkers on his linkedin group (Twitter: @OncologyPharma). This information is clearly vital for cancer patients and their caregivers. In the hope of wider dissemination of this information, I am here summarizing and expanding Nathan's list.
- BRAF mutation V600E is detected in 7% of all cancers; 70% of all malignant melanomas, 63% of papillary thyroid carcinomas, 15% of colorectal tumors. Plexxikon’s PLX4032, a small molecule inhibitor of BRAF-V600E, has shown extremely positive results in the ongoing Phase 2 and 3 melanoma trials.
- c-Kit overexpression predicts response to imatinib (acute lymphocytic leukemia [ALL], CML, GIST)
- DPD = capecitabine
- EGFR/Her1 protein overexpression predict response to cetuximab (Erbitux, ImClone Systems), erlotinib (Iressa), gefitinib or panitumumab (Vectibix, Amgen). Cetuximab or panitumumab binds extracellular domain of EGFR/Her1 with high affinity, block EGFR/Her2 heterodimerization, significantly inhibit EGFR downstream signaling and cell proliferation. These drugs do not help all non–small cell lung cancer (NSCLC) patients due to K-ras mutations which lead to EGFR constituitve signaling bypassing receptor inhibition. Thus, KRAS testing for these two drugs is part of the drug label.. (read: Nature Biotech 2009; 27:110)
- Estrogen receptor (ER-beta) for tamoxifen, exemestane/anastrozole/letrozole (breast cancer)
- G6PD for rasburicase
- Her2/neu (ErbB-2) mutation predicts response to trastuzumab or lapatinib (breast cancer)
- KRAS somatic gene mutations predict response of cetuximab or panitumumab (metastatic colorectal cancer)
- PML/RARα translocation for prescribing arsenic trioxide in leukemias
- BCR-ABL, i.e. Philadelphia chromosome in CML for busulfan, dasatinib, imatinib, nilotinib. Nilotinib is ABL allosteric inhibitor can overcome imatinib-resistance due to certain imatinib-therapy-acquired BCR-ABL mutations.
- Del(5q) for starting lenolidomide therapy in myeloid neoplasias, including myelodysplastic syndrome (MDS) and AML
- CD20 for Rituximab
- CD52 for Alemtuzumab
- CD25 for Denileukin diftitox
Certain genetic variants help identify patient subgroups who may potentially benefit from the choice of a treatment agent or help guide drug dosing regimen and limit toxicity, such as,
- Cytochrome P450 2D6 (CYP2D6) genotype predicts poor tamoxifen response and higher relapse in breast cancer
- CYP3A4 variants predicts dasatinib response in ALL
- DPYD variants predict 5-FU toxicity in breast or colorectal cancer.
- HLA-B*1502 is a marker for adverse cutaneous skin reactions to allopurinol
- Thiopurine methyltransferase (TPMT) genotypes for 6-mercaptopurine, 6-thioguanine and azathioprine to determine optimal treatment for ALL and AML
- UDP-glucuronosyltransferase 1A1 (UGT1A1) genotypes predict toxicity during irinotecan treatment in colorectal cancer treatment. Also for nilotinib. [read here and here]
A report in the October 2010 issue of Journal of National Cancer Institute reminds that clinical adoption of the genomic/genetic testing of these markers has been very slow. However, there are some bright spots. EGFR and KRAS mutation testing is now part of cetuximab and panitumumab drug labels in colorectal cancer. Similarly, ERB2, BCL-ABL and cKIT testing are now routine. But, for many other biomarkers, patients and their families have to be proactive and need to ask! Very few pharmacogenomic biomarkers have been incorporated into routine clinical practice or FDA drug label; without FDA label, many private insurances refuse to cover the cost. The training of clinicians on how to interpret data from pharmacogenomic biomarker testing is another area that needs attention. [read here]
Predictive Biomarkers for Bevacizumab
Bevacizumab (Avastin, Genentech/Roche) is a monoclonal antibody against VEGF-A. It was the very first anti-angiogenic agent approved by the FDA in 2004. Since its introduction in oncology clinical practice, it has benefited thousands of patients with metastatic colon cancer, metastatic NSCLC, metastatic renal cancer and glioblastoma; it is also in clinical trials for many other cancers and is widely prescribed off-label.
In the December 2010 issue of Lancet Oncology (Vol.11, p.112), Adrian Jubb and Adrian Harris of Weatherhall Institute of Molecular Medicine, University of Oxford, UK, reviewed biomarkers for bevacizumab efficacy from multiple trials and concluded that hypertension and VEGF polymorphisms are the only biomarkers that can predict efficacy at present [read here and here]. Unfortunately, there is nothing yet to predict beforehand which patient is a good candidate for initiating bevacizumab therapy.
The company website writes -
"To date, a validated predictive biomarker for Avastin has not been identified, although several candidates have been investigated. Various potential biomarkers in samples from patients in phase III studies of Avastin in mCRC, advanced NSCLC and mBC have been tested for correlation with outcome many of these analyses had low power due to the small sample sizes involved. [read here]

Recently, FDA initiated a process to withdraw bevacizumab's label for metastatic breast cancer due to lack of statistically meaningful improvement in prolonging the life of metastatic breast cancer patients. This decision has been very controversial; most breast cancer foundations and cancer patient advocate organizations oppose FDA action; many insurance companies have said that they will continue to cover bevacizumab use in breast cancer. Meanwhile, in an appeal to FDA, Genentech has proposed a plan to validate VEGF genotype-based biomarkers to identify patients who are likely to obtain significant benefit.

“. . . E2100 showed an improvement in progression-free survival in patients with HER2-negative metastatic breast cancer, but did not show improvements in disease-related symptoms or survival. However, researchers conducted genomic studies within E2100 and identified markers that conferred longer survival and protection against drug-induced hypertension. Specifically, in E2100, researchers uncovered preliminary PGx data linking VEGF-1154 AA and -2578 AA genotypes to an improvement in median overall survival. Additionally, E2100 showed that patients with VEGF-634 CC and -1498 TT genotypes had protection from grade 3-4 hypertension, a common side effect of Avastin. . . . that patients with high levels of plasma VEGF-A who received standard doses of Avastin had a progression-free survival hazard ratio of 0.49. Meanwhile, patients with low levels of VEGF-A had a PFS hazard ratio of 0.86. 'This finding suggests that patients with high levels of VEGF-A may be more likely to derive a more substantial benefit from Avastin,' . . . A spokesperson for Genentech told PGx Reporter that the first-generation test was an ELISA-based assay. 'It suggested that levels of VEGF were a strong prognostic, but not predictive, marker for Avastin’s efficacy,' the spokesperson said. The second-generation test is also an ELISA-based multiplex assay, according to the company representative, which "showed a potential predictive effect of VEGF in metastatic breast cancer and pancreatic cancer for patients with samples available." [read here]
Private-Public-Nonprofit Initiatives
Critical Path Institute, founded in 2005 in Tucson, Arizona, is an independent, non-profit organization dedicated to bringing scientists from the FDA, industry, and academia together to improve the path for innovative new drugs, diagnostic tests and devices to reach patients in need. C-Path’s Predictive Safety Testing Consortium (PSTC) recently reached important milestones in defining biomarkers predicting kidney toxicity.
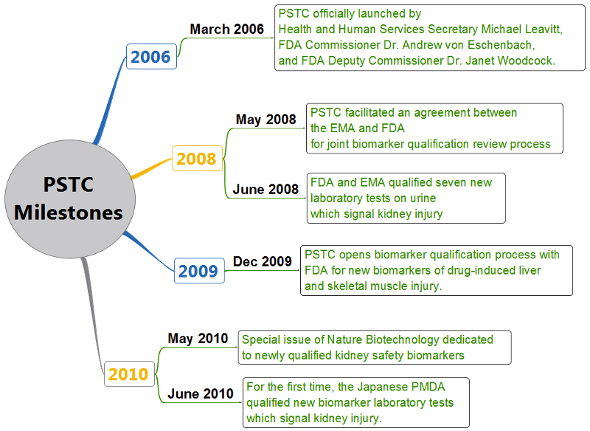
(Nat Biotech. 2010. Volume 28, Issue 5, Articles: p. 432, 436, 441, 444, 446, 455, 463, 470, 478 and 486.
Biomark Med. 2010 Apr;4(2):215-25. Sci Transl Med. 2010 Sep 1;2(47):47ps44) LINK
Olivier Feron in a recent commentary writes:
“It is now clear that in vitro activity is not the bottleneck to the development of such drugs considering the huge amounts of cytotoxic compounds which have been identified along the years. Experimental and preclinical in vivo activity should however not either be considered as the ultimate filter before clinical evaluation. Indeed, many studies using animal models of cancer do report the identification of a critical pathway exquisitely responding to a therapeutic modality based on tumor growth delay measurements or Kaplan–Meier survival curves. These read-outs clearly underestimate the complexity of signaling networks that in fine determine the clinical response to a treatment. Instead, the bottleneck to the development of better anticancer drugs lies in their therapeutic window, i.e., the range between the dosage that gives an anti-tumor effect and the amounts that give more adverse effects than desired effects. The new therapeutic strategies based on targeting antibodies or small molecules are certainly a first step in this direction. [read here or here]
Further Readings and References (Open Access or Free):
- Challenges in pharmacotherapy of neoplastic diseases – the search for addictions by: Olivier Feron. Frontiers in Pharmacotherapy (Sept. 20, 2010) 1:120 [DOI] [FullText]
- AACR-FDA-NCI Cancer Biomarkers Collaborative Consensus Report: Advancing the Use of Biomarkers in Cancer Drug Development. Clin Cancer Res (July 1, 2010) 16; 3299 [DOI][FullText]
- Cancer Pharmacogenomics and Pharmacoepidemiology: Setting a Research Agenda to Accelerate Translation. Andrew N. Freedman et al. JNCI J Natl Cancer Inst (2010) 102 (22): 1698-1705. [DOI][PubMed]
- Pharmacogenetics and pharmacogenomics of anticancer agents. Huang RS, Ratain MJ. CA Cancer J Clin. (2009 Jan-Feb) 59(1):42-55. [DOI][PubMed]
- Paving the Way to Personalized Genomic Medicine: Steps to Successful Implementation. Fackler JL, McGuire AL. Curr Pharmacogenomics Person Med. (Jun 1, 2009) 7(2):125-132.[PubMed][Scholar]
- Chutes and Ladders on the Critical Path:Comparative Effectiveness, Product Value, and the Use of Biomarkers in Drug Development. J Woodcock. Clinical Pharmacology & Therapeutics 86, 12-14 (July 2009)[DOI] (not free acess)
- Assessing the clinical utility of diagnostics used in drug therapy. Woodcock J. Clin Pharmacol Ther. Dec. 2010) 88(6):765-73 [DOI][PubMed]
- The search for a predictive biomarker for Avastin. [Avastin.net] (Accessed Feb. 03, 2010)
- Avastin: Time for a Predictive Test. Analysis & insight: Patricia F. Dimond, Genengnews. Apr 26, 2010[Link]
- Biomarkers for predicting bevacizumab efficacy. Clare Sansom. eCancerMedicalScience.com (Jan 27, 2011) 17:06:51 [Link]
- Biomarkers to predict the clinical efficacy of bevacizumab in cancer. Jubb, A.M. and Harris, A.H. Lancet Oncology (2010) 11, 1172-83. [DOI][Scholar] (not free access)
- Special issue in "Cancers" journal, MDPI Publishing (Basel, Switzerland) expected sometime this year. Special Issue "Biomarkers: Oncology Studies"[Link]
- Regulatory innovation. Steve Usdin and David Flores. BioCentury's 18th Annual Back to School Commentary, Sept 13, 2010 [Link]
For some time, clinicians have been grumbling about not having a biomarker for Avastin or any other anti-angiogenesis compound to better help choose which patients would be most likely to respond, thereby avoiding the need to treat everyone to gain a benefit in a few.
ReplyDeleteSuppose there was a biomarker that was relative to Avastin and could be helpful for predictive purposes? Then you could actually make better use of the drug based on the biomarker. You would be able to predetermine and monitor therapy for specific subtypes and avoid exposing patients to the effects and costs of a drug that may not work for them.
A private cell-based assay lab came along with a smart idea, a rational approach to the problem and some creative thinking to develop a biomarker for anti-angiogenesis compounds.
http://cancerfocus.org/biomarker_for_avastin/46708